blog 1
CBBLE UDHC similar cases
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
55 year old male who is a farmer came to casuality with alleged history of seizure activity on 28/2/22 for which he was admitted in a hospital where he was resuscitated and intubated after having cardiac arrest on day 2 (4 am) of his stay at the hospital.
HISTORY OF PRESENTING ILLNESS :
Patient was apparently asymptomatic 6 years back then he suffered with sudden onset seizure activity which lasted for 8- 10 minutes ON 28/2/2022 .
He had h/o involuntary movements of upper limb and lower limb with uprolling of eyes along with aura ,involuntary micturition and defecation, tongue bite, post ictal confusion.
He was rushed to a nearby hospital and was treated conservatively .During the stay in the hospital patient had cardiac arrest on day 2 of admission at 4 a.m. was intubated and put on mechanical ventilator and referred to us in view of of their affordability issues.
History of fever since 3 days.
PAST HISTORY:
k/c/o seizures since 6 years.
History of trauma to head 10 years back (fall from bike ) ,no chief complaints of LOC, headache, seizures giddiness.
H/o seizure attack 6 years back for which he was treated with levipril.
1 year back he had another seizure activity since then he was advised to take regular medication ( levipil) to avoid future seizure activity but the patient didn't take regular medication.
Not a known case of DM and HTN.
PERSONAL HISTORY:
Alcoholic since 15 years , tobacco smoking since 30 years
GENERAL EXAMINATION:
O/E : patient is on mechanical ventilator
FiO2 - 40%
PEEP- 5
VT - 420
GCS: E1 VT M2
Pallor - present
Icterus absent
Cyanosis - absent
Edema of feet - present
Lymphadenopathy - absent
Clubbing - absent
VITALS:
Temperature: 100 F
BP: 140/80mmhg
PR: 112 bpm
RR : 18CPM
SYSTEMIC EXAMINATION:
CNS:
Pupils - B/L NSRL
Reflexes:
Biceps 2+ 2+
Triceps 2+ 2+
Supinator 2+ 2+
Knee 3+ 3+
Ankle - -
Plantar flexion flexion
CARDIOVASCULAR SYSTEM : S1 and S2 heard, no murmurs heard
RESPIRATORY SYSTEM : BAE present
P/A : soft
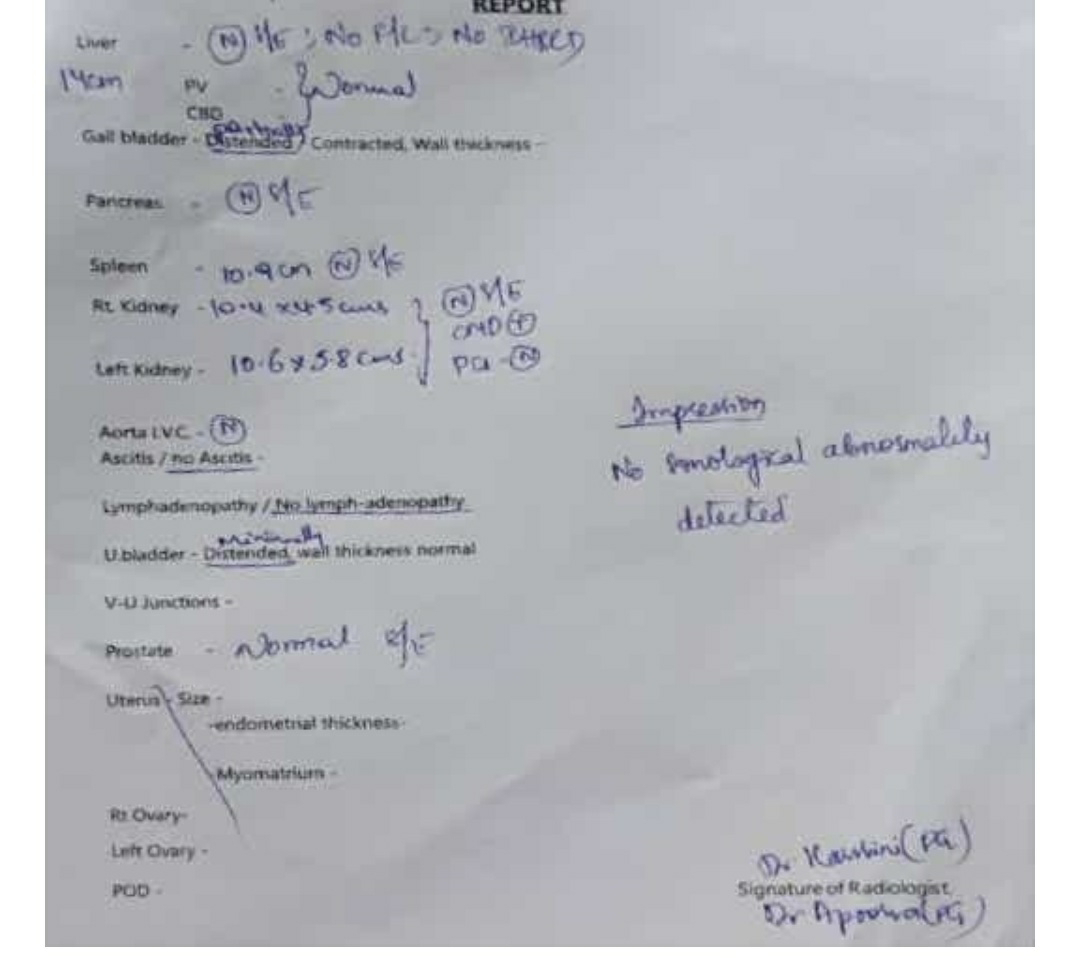
INVESTIGATIONS:


5/3/22
BGT: B POSITIVE
SPOT URINE PROTEIN: 7
SPOT URINE CREATNINE: 74
RATIO: 0.09



PROVISIONAL DIAGNOSIS:
SEIZURE UNDER EVALUATION (? ALCOHOL WITHDRAWAL SEIZURE) ? HYPOXIC ENCEPHALOPATHY POST CPR STATUS DAY 5
TREATMENT:
HEAD AND ELEVATION UP TO 30%
INJ. MEROPENEM 1 G IV BD
INJ. LEVIPIL 500 MG IV BD
INJ MIDAZOLAM 10 MG IN 50 ML NS @ 30 ML/ hr INJ. MANNITOL 100 ML IV BD
INJ. PANTOP 40 MG IV OD
INJ. NEOMOL 100 ML IF TEMPERATURE > 101 F INJ THIAMINE 2 AMP IN ONE DNS IV BD
SOAP NOTES:
DAY 2(7/3/22)

S:- Fever spikes present
O: patient is on mechanical ventilator
PEEP- 5
FiO2 - 40%
VT - 400ml
VITALS:
temp- febrile
BP 140/80 mm hg
PR 130 bpm.
RR 18 cpm
spo2: 92% with Fio2 40%
CVS - S1, S2 heard ,muffled heart sounds
R. :- NVBS Present, no crepts
P/A: soft, non tender
CNS: Pupils :B/L NSRL
REFLEXES : right. left
Biceps 2+ 2+
Triceps . 2+ 2+
Supinator 2+ 2+
Knee - -
Ankle - -
Plantar mute mute
A:- Seizures secondary to ? tuberculoma /NCC ?alcohol with hypoxic encephalopathy with post CPR


status day 7 , mechanical ventilator day 6
nS:- no fever spikes
O- O/E : patient is on mechanical ventilato
PEEP-
FiO2 - 40%
VT - 400m
Timp : 2.
VITALS
temp- afebril
BP: 110/90mm hg
PR: 115 bpm.
RR: 16 cpm
spo2: 99% with Fio2 40
GRBS: 168 mg/d
CVS - S1, S2 heard ,no murmur
RS. :- NVBS Present, no crept
P/A: soft, non tender
CNS: Pupils :B/L NSRL
GCS: E1VTM
Cough reflex presen
corneal reflex presen
conjunctival reflex presen
REFLEXES : right. left
Biceps 2+
Triceps . 2+ 2
Supinator 2+ 2
Knee 3+ 3+
Ankle -
Plantar mute mut
A: Seizures secondary to ? tuberculoma /NCC ?alcohol with hypoxic encephalopathy with post CPR status day 8 , mechanical ventilator day
P: ENT opinion i/v/o tracheostom
y7e- ++- ttt2 ssl% e:1l 5r



S:- fever spikes present
O- O/E : patient is on mechanical ventilator
PEEP- 5
FiO2 - 40%
VT - 400ml
Timp : 2.1
VITALS:
temp- 100.9 F
BP: 120/90mm hg @ NORAD 6ml /hr
PR: 114 bpm.
RR: 16 cpm
spo2: 99% with Fio2 40%
GRBS: 129 mg/dl
CVS - S1, S2 heard ,no murmurs
RS. :- NVBS Present, no crepts
P/A: soft, non tender
CNS: Pupils :B/L NSRL
GCS: E1VTM1
Cough reflex present
corneal reflex present
conjunctival reflex present
REFLEXES : right. left
Biceps 2+ 2+
Triceps . 2+ 2+
Supinator 2+ 2+
Knee 3+ 3+
Ankle - -
Plantar extensor extensor
A: Seizures secondary to ? tuberculoma /NCC ?alcohol with hypoxic encephalopathy with post CPR status day 9 , mechanical ventilator day 8




Comments
Post a Comment